 Once again, research shows that a supplement is not beneficial and may have some health harms, while eating foods rich in the mineral or vitamin being measured has health benefits. A ten year study found that calcium supplements are not beneficial and linked to health harm - they raised the risk of atherosclerosis, as measured by "coronary artery calcification" or plaque buildup in arteries, while a diet high in calcium rich foods was linked with health benefits (a protective effect). Other studies have found a higher risk for other health problems with calcium supplements (heart attacks, kidney stones, death),
Once again, research shows that a supplement is not beneficial and may have some health harms, while eating foods rich in the mineral or vitamin being measured has health benefits. A ten year study found that calcium supplements are not beneficial and linked to health harm - they raised the risk of atherosclerosis, as measured by "coronary artery calcification" or plaque buildup in arteries, while a diet high in calcium rich foods was linked with health benefits (a protective effect). Other studies have found a higher risk for other health problems with calcium supplements (heart attacks, kidney stones, death),
Currently an estimated 43 percent of American adults take a supplement that includes calcium. Instead, for health benefits, focus on eating calcium rich foods. Some calcium rich foods are: dairy products (milk, cheese, yogurt, kefir), sardines, salmon, broccoli, collard greens, kale, edamame, figs, oranges, white beans, okra, tofu, and almonds. From Science Daily:
Calcium supplements may damage the heart
After analyzing 10 years of medical tests on more than 2,700 people in a federally funded heart disease study, researchers at Johns Hopkins Medicine and elsewhere conclude that taking calcium in the form of supplements may raise the risk of plaque buildup in arteries and heart damage, although a diet high in calcium-rich foods appears be protective.
In a report on the research....the researchers caution that their work only documents an association between calcium supplements and atherosclerosis, and does not prove cause and effect. But they say the results add to growing scientific concerns about the potential harms of supplements....But our study adds to the body of evidence that excess calcium in the form of supplements may harm the heart and vascular system.
"The researchers were motivated to look at the effects of calcium on the heart and vascular system because studies already showed that "ingested calcium supplements -- particularly in older people -- don't make it to the skeleton or get completely excreted in the urine, so they must be accumulating in the body's soft tissues," says nutritionist John Anderson, Ph.D., professor emeritus of nutrition at the University of North Carolina at Chapel Hill's Gillings School of Global Public Health and a co-author of the report. Scientists also knew that as a person ages, calcium-based plaque builds up in the body's main blood vessel, the aorta and other arteries, impeding blood flow and increasing the risk of heart attack.
Their study focused on 2,742 of these participants who completed dietary questionnaires and two CT scans spanning 10 years apart. The participants chosen for this study ranged in age from 45 to 84, and 51 percent were female. Forty-one percent were white, 26 percent were African-American, 22 percent were Hispanic and 12 percent were Chinese. At the study's onset in 2000, all participants answered a 120-part questionnaire about their dietary habits to determine how much calcium they took in by eating dairy products; leafy greens; calcium-enriched foods, like cereals; and other calcium-rich foods....The coronary artery calcium tests were repeated 10 years later to assess newly developing or worsening coronary heart disease.
Next, the investigators focused on the differences among those taking in only dietary calcium and those using calcium supplements. Forty-six percent of their study population used calcium supplements. The researchers.....found that supplement users showed a 22 percent increased likelihood of having their coronary artery calcium scores rise higher than zero over the decade, indicating development of heart disease....Among participants with highest dietary intake of calcium -- over 1,022 milligrams per day -- there was no increase in relative risk of developing heart disease over the 10-year study period.
Excerpts from the original study (Please note: CVD = cardiovascular disease, CAC = coronary artery calcification) in the Journal of the American Heart Association: Calcium Intake From Diet and Supplements and the Risk of Coronary Artery Calcification and its Progression Among Older Adults: 10‐Year Follow‐up of the Multi‐Ethnic Study of Atherosclerosis (MESA)
Recent evidence derived from randomized, controlled trials, including the Women's Health Initiative, have raised a concern for an association between calcium supplement use and increased risk for CVD events.12, 13, 14 Among calcium supplement users, a high intake of calcium greater than 1400 mg/day has been reported to be associated with higher death rates from all causes, including from CVD.15
The purported CVD risk associated with total calcium intake may depend on the source of calcium intake.3 Intake of calcium from food sources has not been shown to increase CVD risk, whereas a signal for increased risk of myocardial infarction (MI) among calcium supplement users has been reported.7 In a similar fashion, dietary calcium intake may decrease risk of kidney stones, whereas calcium supplementation may increase risk.16 One explanation for this apparent paradox may be that large boluses of calcium intake through supplements may transiently elevate serum calcium concentrations,17, 18 which, in turn, may lead to vascular calcification and other adverse health effects.
In summary, results from this long‐term study of 10 years showed a protective relationship between total calcium intake and incident coronary atherosclerosis, particularly among nonsupplement users. Even though mean total calcium intake in quintile 5 was greater than the upper limits of current recommendations, no increased risk of CAC progression was found, and the highest quintile of calcium intake actually had decreased risk of incident CAC among those without prevalent CAC at baseline. However, we found evidence that calcium supplement use was independently associated with incident CAC, whether or not we adjusted for total calcium intake.
 We all know that exercise is beneficial for health. Research suggests that exercising out in nature is best for several varied reasons - including that it
We all know that exercise is beneficial for health. Research suggests that exercising out in nature is best for several varied reasons - including that it  The
The 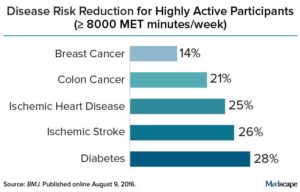 Credit: Medscape
Credit: Medscape Another interesting study looking at whether being overweight is linked to premature death, heart attacks, and diabetes. This study looked at sets of twins, in which one is heavier than the other, and followed them long-term (average 12.4 years) and found that NO - being overweight or obese (as measured by Body Mass Index or BMI) is NOT associated with premature death or heart attack (myocardial infarction), but it is associated with higher rates of type 2 diabetes. These results are in contrast with what
Another interesting study looking at whether being overweight is linked to premature death, heart attacks, and diabetes. This study looked at sets of twins, in which one is heavier than the other, and followed them long-term (average 12.4 years) and found that NO - being overweight or obese (as measured by Body Mass Index or BMI) is NOT associated with premature death or heart attack (myocardial infarction), but it is associated with higher rates of type 2 diabetes. These results are in contrast with what  Studies have found that increased nut consumption has been associated with
Studies have found that increased nut consumption has been associated with  Yup, according to a new mega-study, being overweight or obese is linked to higher risk of dying prematurely than being normal weight. And the more you weigh, the greater the risk.
Yup, according to a new mega-study, being overweight or obese is linked to higher risk of dying prematurely than being normal weight. And the more you weigh, the greater the risk.  Previous research on the health benefits of eating fish, fish oil supplements, and other sources of omega-3 fatty acids has shown mixed
Previous research on the health benefits of eating fish, fish oil supplements, and other sources of omega-3 fatty acids has shown mixed  A second study was just published about the benefits of eating whole grains daily - again a significantly lower risk of premature death, and again the effects were dose-related. That is, the more whole grains eaten daily, the lower the risk of early death. Like the
A second study was just published about the benefits of eating whole grains daily - again a significantly lower risk of premature death, and again the effects were dose-related. That is, the more whole grains eaten daily, the lower the risk of early death. Like the