 Once again a study looked at biofilms in sinuses - but this time in the sinuses of healthy people and not those with sinusitis. Various different species of bacteria and small size "microcolonies" or biofilms were found in the healthy maxillary sinuses of all 30 people - so yes, it appears that the presence of biofilms in the sinuses is normal in healthy people. And yes, the presence of bacteria (even some low levels of species which are typically associated with sinusitis) are normally found in the sinuses of healthy people. (Earlier research also found this last finding.)
Once again a study looked at biofilms in sinuses - but this time in the sinuses of healthy people and not those with sinusitis. Various different species of bacteria and small size "microcolonies" or biofilms were found in the healthy maxillary sinuses of all 30 people - so yes, it appears that the presence of biofilms in the sinuses is normal in healthy people. And yes, the presence of bacteria (even some low levels of species which are typically associated with sinusitis) are normally found in the sinuses of healthy people. (Earlier research also found this last finding.)
The researchers state that it is normal for people to have "small size bacterial microcolonies" (of different kinds of bacteria) in the sinuses. The researchers theorized that the biofilms are probably "in equilibrium" under the influence of "inhibiting defensive factors of the body", but they can become a source of infection if there are favorable conditions (such as illness). In other words, the researchers said that these biofilms are more like "bacteria films" in that they contain bacteria, but they live in small colonies that don't cause an inflammatory response with sinusitis symptoms.
One negative of this study was that advanced genetic sequencing was not done on the samples. Instead all samples taken from the people were cultured, which we now know misses a lot of bacterial and other microbial species (fungi, viruses). They looked at the microcolonies (biofilms) with scanning microscopes. Thus, while they found an assortment of bacteria on the sinuses of each person - they only found a total of 41 bacterial species among 30 persons. This is in contrast to studies using modern genetic sequencing that found hundreds of microbial species in healthy sinus microbiomes (microbial communities).
The other issue is that it is not clear to me if there were biofilms or microcolonies that contained "beneficial" species in any of the samples. Other research suggests that biofilms of beneficial bacteria are also found in humans, and that this is one way beneficial bacteria that normally can't survive with exposure to oxygen can survive oxygen (the slime coating on the colony protects the bacteria within).
Other studies also stress that in healthy people there is "homeostasis" or "equilibrium" among all the microbes living in the sinuses, - a microbial community (which includes biofilms), and which helps maintain sinus health. See post with discussion of Mackenzie et al 2017 study: "A stable network of microbial interactions, established through processes such as niche competition, nutrient cycling, immune evasion, and biofilm formation help maintain homeostasis during health." But, as has been usual in recent sinus research, the current study also stated that much is unknown, that there are theories which are not yet proven one way or another, and more research needs to be done. Of course.... Excerpts from Morawska-Kochman et al research article in PLoS ONE:
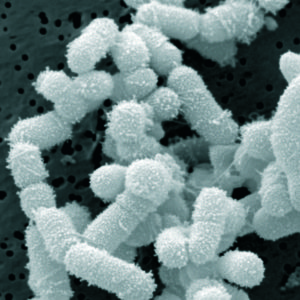
The presence of bacterial microcolonies on the maxillary sinus ciliary epithelium in healthy young individuals
The aim of this cross-sectional in vitro study was to evaluate the mucosal surfaces of healthy maxillary sinuses, explore different forms of bacterial microorganism colonies present on the mucous membrane, and determine a mucosal surface area they occupy. Samples of the maxillary sinus mucosa were collected from 30 healthy patients (M = 11; F = 19). The material was obtained during the Le Fort I osteotomy performed during corrective jaw surgery. The morphological and morphometric analysis of sinus mucosa and bacterial film that was grown on it was performed using scanning electron microscopy (SEM) as well as imaging software.
Scanning electron microscopy analysis showed the presence of different bacterium and bacteria-like structures in all the analyzed samples. In most cases, the bacterial film was mostly composed of diplococci-like and streptococci-like structures on the mucosa of the paranasal sinus. In any case, the mucous layer did not cover the whole lining of the evaluated sample. Each colony consists of more than 20 single bacterial cells, which has grown in aggregates.
Under the conditions of normal homeostasis of the body, the maxillary sinuses present diverse bacterial colonization. The bacteria are dispersed or concentrated in single microcolonies of the biofilm on the border of the mucous covering the ciliary epithelium. There is no uniform layer of the biofilm covering the mucosa of the maxillary sinuses. Because the biofilm is detected on healthy individuals sinus mucosa, the clinical question if it may become pathogenic is unclear and require an explanation.
It should also be noted that pathogenic organisms, such as Pseudomonas aeruginosa, Haemophilus influenzae, Streptococcus pneumoniae, or Staphylococcus aureus can be found in patients without active symptoms of the disease. Usually, colonization is defined as the presence of bacteria on the mucous membrane, and the lack of the inflammatory response distinguishes it from an infection.
However, the bacteria film in contrast to typical biofilm might be defined by the presence of bacteria, that growth in colonies without inducing the inflammatory response. Thus, the aim of the study was to evaluate the mucosal surfaces of the healthy maxillary sinuses (without any history of recent acute sinus inflammations or chronic inflammation in the past), to identify different forms of bacterial microorganisms which could, under certain conditions, become opportunistic or pathogenic and determine a mucosal surface of the area they occupy.
Scanning electron microscope investigations revealed the presence of bacterial film on the surface of maxillary sinus mucosa in 30 patients. Moreover, microbiological examinations of specimens taken from study participants revealed the presence of various types of aerobic and anaerobic bacteria in 28 cases (93.34%) out of 30 studied samples. All samples had mixed flora. In total, 41 different microorganisms were isolated. The most frequently found microorganism was Streptococcus spp. in over 90% of all samples, while Propionibacterium acnes were present in 29,2% of samples, and Staphylococcus spp. was present in 17% of the samples.
Scanning electron microscopy analysis showed that the mucous layer has a thickness of 200 nm (± 40), which is covered up to 5% of the surface of each sample. The analysis showed the presence of bacteria-like microcolony structures in all analyzed samples.....Each colony consisted of more than 20 single bacterial cells, that had grown in aggregates. These clearly indicate the existence of a bacterial-like microcolony on maxillary sinus mucosa.

Bacterial microcolonies on the maxillary sinus ciliary epithelium in healthy young individuals. Credit: Morawska-Kochman et al.


 sinusitis
sinusitis 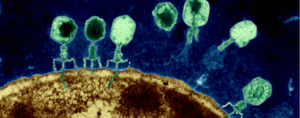 Some researchers are now testing to see if phage therapy could be a possible treatment for some conditions, such as chronic sinusitis and wound infections. Phage therapy, which uses
Some researchers are now testing to see if phage therapy could be a possible treatment for some conditions, such as chronic sinusitis and wound infections. Phage therapy, which uses  Interesting, but in some ways horrifying - the hidden world of microbes teeming around us. With new techniques such as genetic sequencing we now know that at least a couple of thousand different species live in our water pipes in
Interesting, but in some ways horrifying - the hidden world of microbes teeming around us. With new techniques such as genetic sequencing we now know that at least a couple of thousand different species live in our water pipes in  Even though this study was done in a laboratory, it gives further support for the treatment of sinusitis with bacteria and other microbes. And it could help explain why repeated courses of antibiotics don't "cure" many chronic infections - because biofilms filled with pathogenic bacteria are signs of microbial communities out-of-whack. Which is why my family's successful chronic sinusitis treatment with kimchi (juice) containing Lactobacillus sakei is all the more impressive. From Science Daily:
Even though this study was done in a laboratory, it gives further support for the treatment of sinusitis with bacteria and other microbes. And it could help explain why repeated courses of antibiotics don't "cure" many chronic infections - because biofilms filled with pathogenic bacteria are signs of microbial communities out-of-whack. Which is why my family's successful chronic sinusitis treatment with kimchi (juice) containing Lactobacillus sakei is all the more impressive. From Science Daily:
 I spent time this past week searching the medical literature (US National Library of Medicine - Medline/PubMed) for the latest in sinusitis research. I wish I could tell you that amazing research has been happening recently, especially with the sinus microbiome (which could mean treating sinusitis with microbes), but I was disappointed. Really disappointed.
I spent time this past week searching the medical literature (US National Library of Medicine - Medline/PubMed) for the latest in sinusitis research. I wish I could tell you that amazing research has been happening recently, especially with the sinus microbiome (which could mean treating sinusitis with microbes), but I was disappointed. Really disappointed. Injection of fillers: Side effects in the form of stubborn, tender lumps or even lesions are becoming an increasing problem. Photo credit: University of Copenhagen
Injection of fillers: Side effects in the form of stubborn, tender lumps or even lesions are becoming an increasing problem. Photo credit: University of Copenhagen