 A thought-provoking article by Heiman and Greenway was just published in the journal Molecular Metabolism making the case that changes in farming practices over the last 50 years have resulted in decreased agricultural diversity which, in turn, has resulted in decreased dietary diversity, and that the reduction in dietary diversity has changed and decreased the richness of the human gut microbiota (microbes living in the gut). And meanwhile, during the past 50 years, the rates of obesity, type 2 diabetes, and inflammatory bowel diseases sharply increased - and in each of these conditions there is a reduction of the gut microbial diversity. Similar views have also been stated by others in the field of microbiology.
A thought-provoking article by Heiman and Greenway was just published in the journal Molecular Metabolism making the case that changes in farming practices over the last 50 years have resulted in decreased agricultural diversity which, in turn, has resulted in decreased dietary diversity, and that the reduction in dietary diversity has changed and decreased the richness of the human gut microbiota (microbes living in the gut). And meanwhile, during the past 50 years, the rates of obesity, type 2 diabetes, and inflammatory bowel diseases sharply increased - and in each of these conditions there is a reduction of the gut microbial diversity. Similar views have also been stated by others in the field of microbiology.
The thinking is that the more diverse the diet, the more diverse the gut microbiome (and healthier), and the more it can adapt to disturbances. Heiman and Greenway state: "Unfortunately, dietary diversity has been lost during the past 50 years because of economic pressures for greater food production to support a growing world population.... Of the 250,000 to 300,000 known edible plant species, humans use only 150 to 200...Today, 75 percent of the world's food is generated from only 12 plants and five animal species."
Also, agricultural practices of using antibiotics as growth promoters for poultry, swine, and cattle further harm the human gut microbiome when the meat is ingested by humans, and pesticide residues on crops ingested by humans may have gut microbiome effects. Even emulsifiers, used in processed foods, reduce microbial richness. Every time a person goes on a certain diet (vegan, Paleo, etc) or makes dietary choices in which some foods are eliminated, it makes it easier for some microbial species, and gives them a competitive advantage over other gut microbes. From Science Daily:
Reduction in dietary diversity impacts richness of human gut microbiota
Changes in farming practices over the last 50 years have resulted in decreased agro-diversity which, in turn, has resulted in decreased dietary diversity. The significant impact of this change in dietary richness on human health is an emerging topic for discussion
Heiman and Greenway describe how the reduction in dietary diversity has changed the richness of human gut microbiota, the community of microorganisms living in the gut. The researchers point out that healthy individuals have diverse gut microbiota and many of the common pathologies of the 21st century, including type 2 diabetes, obesity and inflammatory bowel disease, are associated with reduced microbiotic richness.
Gut microbiota function as an endocrine organ, metabolizing specific nutrients from the diet and producing specific substances that act as metabolic signals in the host. It follows then that highly specialized diets will change the landscape of the gut microbiome over time. In fact, it takes only a few days of changing diet to alter the microbiotic makeup of the human gut. And if the dietary change involves elimination of one or more macronutrients (think Atkins or Paleo or vegan), humans are essentially selecting for some microbiotic species over others.
The importance of microbiota diversity cannot be overstated. They produce an abundance of important molecules for the host and with increased variation comes increased adaptability and an increased range of physiological responses. "The greater the repertoire of signals, the more likely is the ability to maintain homeostasis when dietary intake is perturbed," explain Heiman and Greenway. "Furthermore, because each particular macronutrient has the potential to be metabolized by microbiota into unique metabolic signals, the greater the variety in signals, the greater the variety of responses possible."
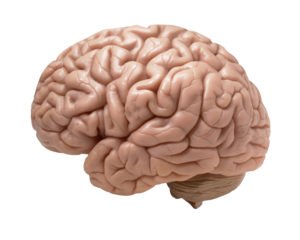 Another study showing that higher physical activity (from a variety of activities) is "related to larger gray matter volume in the elderly, regardless of cognitive status", specifically in gray matter areas of the brain responsible for memory, learning, and cognition. In other words, higher levels of physical activity reduce brain atrophy that occurs with aging and improves cognitive function in elderly individuals. There is also discussion of higher activity levels improving cerebral (brain) blood flow. Bottom line: get off your butt and move more for better brain health. From Medical Xpress:
Another study showing that higher physical activity (from a variety of activities) is "related to larger gray matter volume in the elderly, regardless of cognitive status", specifically in gray matter areas of the brain responsible for memory, learning, and cognition. In other words, higher levels of physical activity reduce brain atrophy that occurs with aging and improves cognitive function in elderly individuals. There is also discussion of higher activity levels improving cerebral (brain) blood flow. Bottom line: get off your butt and move more for better brain health. From Medical Xpress: Not good news. More than half of Americans’ calories come from “ultra-processed foods,” according to
Not good news. More than half of Americans’ calories come from “ultra-processed foods,” according to  Yes, the chemicals in personal care products and cosmetics you use absolutely get into your body, have effects, and can be measured in the urine. Of especially big concern are the endocrine (hormone) disrupting chemicals such as phthalates, parabens, triclosan, and oxybenzone (BP-3). This study shows that even taking a 3 day break from these chemicals lowers their levels in your body. The researchers found that : "The adolescent girls in this study experienced an average within girl decline of 27-45% in urinary concentrations of certain phthalates, certain parabens, triclosan, and oxybenzone after three days of abstaining from conventional personal care products and using replacement products with labels indicating they did not contain these chemicals."
Yes, the chemicals in personal care products and cosmetics you use absolutely get into your body, have effects, and can be measured in the urine. Of especially big concern are the endocrine (hormone) disrupting chemicals such as phthalates, parabens, triclosan, and oxybenzone (BP-3). This study shows that even taking a 3 day break from these chemicals lowers their levels in your body. The researchers found that : "The adolescent girls in this study experienced an average within girl decline of 27-45% in urinary concentrations of certain phthalates, certain parabens, triclosan, and oxybenzone after three days of abstaining from conventional personal care products and using replacement products with labels indicating they did not contain these chemicals." For years stores and manufacturers have promoted the advantages of Scotchgard and Teflon nonstick coatings for pots and pans, as stain-proofing for upholstered furniture and rugs, as a water repellent for clothing, for consumer goods such as dental floss, and for grease-proof food wrappers and containers. And yes, people have been convinced - with most cookware sold today being of the nonstick type, and the popularity of sofas and rugs coated with non-stain coatings. But once again, chemicals come with a price and health effects, and unfortunately these particular chemicals are found in all of us in varying levels.
For years stores and manufacturers have promoted the advantages of Scotchgard and Teflon nonstick coatings for pots and pans, as stain-proofing for upholstered furniture and rugs, as a water repellent for clothing, for consumer goods such as dental floss, and for grease-proof food wrappers and containers. And yes, people have been convinced - with most cookware sold today being of the nonstick type, and the popularity of sofas and rugs coated with non-stain coatings. But once again, chemicals come with a price and health effects, and unfortunately these particular chemicals are found in all of us in varying levels. Flame retardants. All around us, and in us. So, so hard to avoid because they're in electronic goods, in upholstered furniture, polyurethane foam, carpet pads, some textiles, the foam in baby items, house dust, building insulation, and on and on. And unfortunately, while a number of toxic flame retardants have been phased out, it appears that the new replacements may be just as bad and are more easily inhaled (the small particles go down the air tract and into the lung tissue).
Flame retardants. All around us, and in us. So, so hard to avoid because they're in electronic goods, in upholstered furniture, polyurethane foam, carpet pads, some textiles, the foam in baby items, house dust, building insulation, and on and on. And unfortunately, while a number of toxic flame retardants have been phased out, it appears that the new replacements may be just as bad and are more easily inhaled (the small particles go down the air tract and into the lung tissue).
 Two new papers just published in the British Journal of Nutrition are analyses of existing studies that compare conventional vs organic milk, and conventional vs organic red meat. Both studies found clear differences between organic meat and milk compared to conventional milk and meat, with the organic milk and meat best health-wise, especially due to differences in
Two new papers just published in the British Journal of Nutrition are analyses of existing studies that compare conventional vs organic milk, and conventional vs organic red meat. Both studies found clear differences between organic meat and milk compared to conventional milk and meat, with the organic milk and meat best health-wise, especially due to differences in  The finding that the oral bacteria Streptococcus mutans, which is found in 10% of the population, is linked with hemorrhagic strokes is big. S. mutans is found in tooth decay or cavities (dental caries). The researchers found a link with cnm-positive S. mutans with both intracerebral hemorrhage (ICH) and also with cerebral microbleeds.
The finding that the oral bacteria Streptococcus mutans, which is found in 10% of the population, is linked with hemorrhagic strokes is big. S. mutans is found in tooth decay or cavities (dental caries). The researchers found a link with cnm-positive S. mutans with both intracerebral hemorrhage (ICH) and also with cerebral microbleeds.